Microbiology Cheat Sheet: Key Concepts & Study Notes
Microbiology Cheat Sheet Prep

Finish by April 8th
5-10 Key Points/Notes for Each Week (Less if Including Pictures)
Please Use Only Information Directly from the Textbook
Chapter 13: Antimicrobial Control & Therapeutics
Sterilization vs. Disinfection
- Sterilization: Complete eradication of all viable microorganisms, including bacteria, viruses, fungi, and spores. Methods include:
- Autoclaving (high pressure and temperature)
- Pasteurization (moderate heat)
- Cold methods (refrigeration and freezing)
- Filtration (physical removal)
- Irradiation (ionizing radiation)
- Chemical sterilants
- Disinfection: Reduction of microbial populations to safe levels, significantly reducing pathogens and infection risk.
Antimicrobial Agents
- Categorized as:
- Cidal agents: Directly kill microorganisms.
- Static agents: Inhibit growth and reproduction.
- Mechanisms of action include disrupting cell walls, interfering with protein synthesis or nucleic acid replication, or disrupting metabolic processes.
Chemical Disinfectants
- Widely used for surface disinfection in healthcare, food processing, etc.
- Efficacy influenced by concentration, contact time, pH, temperature, and organic matter.
- Common disinfectants: chlorine compounds (bleach), alcohol-based solutions, quaternary ammonium compounds (quats), phenolic compounds, hydrogen peroxide, iodine-based solutions.
Modes of Action and Microbial Spectrum
- Antibiotics exhibit selective toxicity by targeting unique bacterial cell structures or enzymes.
- Targets include cell wall synthesis, cell membrane integrity, DNA/RNA synthesis, protein synthesis, and metabolism.
- Antibiotics interfere with peptidoglycan synthesis, DNA replication, transcription, and protein synthesis.
Empirical vs. Targeted Therapy
- Empirical therapy: Antibiotics prescribed based on likely pathogens before culture results.
- Targeted therapy: Antibiotics selected based on culture and susceptibility testing.
- Combination therapy may be used for synergistic effects or broader coverage.
Synergism in Infection Treatment
- Synergistic antibiotic combinations enhance effectiveness beyond the additive effect.
- Examples: Aminoglycosides and vancomycin target different stages of bacterial protein synthesis.
- Antagonistic interactions should be avoided as they decrease effectiveness.
Selective Toxicity and Antibiotic Resistance
- Selective toxicity targets bacterial processes absent in human cells.
- Resistance mechanisms (e.g., beta-lactamase production, altered penicillin-binding proteins) can render antibiotics ineffective.
- Understanding selective toxicity and resistance guides the development of new antibiotics.
Chapter 14: Human Microbiome in Health & Disease
- Bioburden: The number of microorganisms found in the human body.
- Virome: Viruses that are part of the human body (or the microbiome).
- Skin:
- Acidic pH (4-6) inhibits microbial growth.
- Contains lysosomes that degrade bacterial peptidoglycan.
- Normal skin flora: Staphylococcus epidermidis, Bacillus species, and Candida species (yeast).
- Cutibacterium acnes: Causes acne; oils in our skin promote inflammation, potentially forming blackheads.
- The Eye:
- Antimicrobial factors like lysozyme inhibit colonization.
- Pink eye (conjunctivitis) is caused by Haemophilus influenzae, leading to inflammation.
- Oral and Nasal Cavities:
- Infant’s mouth colonized by non-pathogenic Neisseria species.
- Streptococcus mutans: Attaches to tooth enamel.
- Streptococcus salivarius: Binds to gingival surfaces, producing a polysaccharide called glycocalyx that allows bacterial adherence.
- Nasopharynx and Oropharynx: Contain Staphylococcus aureus and Staphylococcus epidermidis.
- Dental procedures can cause organisms to enter the bloodstream (bacteremia), a problem for those with heart issues.
- Vegetations (biofilms made from bacterial cells) can form on heart valves.
- Respiratory Tract (RT):
- Mucociliary escalator helps move particles out of the lungs.
- Streptococcus pneumoniae infection can overwhelm this system.
- Stomach:
- Acidic environment can kill bacteria, especially Vibrio cholerae.
- Malnourished individuals may have reduced stomach acidity, increasing susceptibility to infection.
- The Intestine:
- Alkaline environment.
- Allows colonization of mostly Gram-positive bacteria like Firmicutes and Actinobacteria.
- Less bile content promotes bacterial growth.
- General:
- Breastfeeding microbiome: Bifidobacterium helps protect against intestinal pathogens.
- Abundant gut bacteria: Faecalibacterium prausnitzii (responsible for fermentation).
- Obesity and Microbiota: Obese individuals may have more hydrogen-using and methane-producing archaea, which are responsible for slow fermentation.
- Genitourinary (GU) Tract:
- Distal urethra contains Staphylococcus epidermidis.
- Imbalance in microbiomes can result in yeast infections caused by Candida albicans.
Chapter 17: Immunization and Vaccines
Active Immunization (Vaccines): Injection of antigen to stimulate the immune system, producing antigen-specific antibodies and T-cells.
Passive Immunization (Antitoxins): Administration of protective antibodies, also acquired through breastfeeding.
Effective Vaccine Characteristics
- Does not harm the vaccinated individual and does not require many boosters.
- Stimulates B-cell and T-cell responses.
- Results in long-term immunological memory.
- Protects against the natural pathogen.
Killed or Inactivated Vaccines (IM)
Uses dead organisms with intact antigenicity.
- Advantages:
- No reversion to virulence.
- Relatively stable shelf life.
- Disadvantages:
- High production costs.
- Examples: Hepatitis A, Influenza, Rabies, Polio.
Live or Attenuated Vaccines (SubQ, PO)
Uses organisms mutated for growth in the host only, mimicking infection for stronger immunity.
- Advantages:
- Low preparation cost.
- Elicits the desired immunological response.
- Usually, a single dose is sufficient.
- Disadvantages:
- Potential to revert to virulence.
- Limited shelf life.
- Examples: HIV, MMR, Adenovirus, Rotavirus, Varicella, Shingles.
Purified Component Vaccines (IM)
Uses antigenic subunits of an infectious agent (acellular or toxoid).
- Toxoids: Diphtheria, Tetanus, Pertussis, Botulism.
- Subunits: Hepatitis B, HPV, Influenza.
Conjugated Vaccines
Link a highly immunogenic protein (e.g., diphtheria toxoid) with a poorly immunogenic capsule polysaccharide (e.g., Haemophilus influenzae type b) to boost the immune response.
DNA or RNA Vaccines
Involves injection of DNA/RNA encoding antigen into muscle (not yet commercially available).
Herd Immunity
Occurs when a large portion of the population is immunized against contagious diseases transmitted between humans.
Opposition to Vaccines
Reactions to vaccines are typically low to none, with mild fever or soreness at the injection site being the most common.
Chapter 18: Microbial Pathogenesis
Pathogenicity and Pathogen Evolution
Pathogenesis: How pathogens cause disease by entering the host, attaching, avoiding immunity, and exiting.
- Pathogens are characterized by virulence factors (traits that help cause disease, such as pili).
Pathogenicity Island: A genomic island containing virulence factors, potentially transferred from another genome.
Genomic Island: A DNA region with properties indicating transfer from another genome.
Pathogenicity Genes vs. Pathogenicity Islands
| Pathogenicity Genes | Pathogenicity Islands |
|---|---|
|
|
Horizontal Gene Transfer and Pathogen Evolution
- Describes major cellular tools microbes use to cause disease.
- Discusses strategies pathogens use to survive in a host.
- Compares pathogenic mechanisms of viral, bacterial, fungal, and protozoan pathogens.
Attachment to Host Cells
- Explains why pathogens need to attach to host cells.
- Describes various microbial attachment techniques.
- Differentiates the structure and function of type I and type IV pili.
- Discusses the role of biofilms in pathogenicity.
Surviving Within a Host
- Explains how pathogens distinguish between intracellular and extracellular existence.
- Describes strategies pathogens use to avoid the immune system.
- Distinguishes extracellular pathogens from facultative and obligate intracellular pathogens.
- Discusses three main ways intracellular pathogens avoid intracellular destruction.
Host Damage and Manipulation
- Describes nine basic cellular targets for bacterial toxins.
- Explains the modes of action for staphylococcal alpha toxin, cholera toxin, diphtheria toxin, Shiga toxin, and anthrax toxin.
- Differentiates endotoxin from exotoxin.
- Describes secretion systems pathogens use to export exotoxins/effector proteins.
- Discusses the evolutionary relationships between secretion systems and other microbial structures.
Viral Pathogenesis
- Discusses antigenic variation in rhinovirus and influenza viruses.
Chapter 19: Skin and Eye Infections
- Forms of rashes include: 1) Macules [flat, red], 2) Papules [solid, elevated], 3) Vesicles [fluid-filled], 4) Pustules [pus-filled].
- Viral Infections of the Skin: Measles/Rubeola (Koplik spots, maculopapular rash) — German measles/Rubella (maculopapular rash) — Erythema infectiosum/Fifth disease (slapped-cheek rash) — Roseola infantum/Exanthem subitum/Sixth disease (maculopapular rash, erythematous tympanic membrane) — Chickenpox (pruritic vesicular rash); Shingles (painful vesicular rash) — Cold sores (blisters of mouth or genitals) — Common warts/Verruca vulgaris (small hard growths) — Hand, foot, and mouth disease (painful, oral lesions, rash on palms and soles) — Smallpox (enanthem on oral mucosa and pustular, red, crusted enanthem on skin).
- Bacterial Infections of the Skin: Staphylococcal: Folliculitis (hair follicle), furuncle/boil (abscess of hair follicle), carbuncle (draining mass), scalded skin syndrome (generalized peeling in infants) — Necrotizing fasciitis (flesh-eating, rapidly progressing cellulitis) — Erysipelas (orange peel) — Cellulitis (red, hot, swollen, tender) — Acne — Impetigo (weeping small papular lesions and crust).
- Fungal Infections of the Skin: Dermatophytosis (dry, scaly lesion, named after location) — Tinea versicolor (Malassezia, small, flat, discolored lesion, variable colors, no itch) — Candidiasis (patchy, smooth-looking lesions, infects where skin rubs).
- Skin Infections of Special Circumstance: Burn infections (pus, possibly with green hue from Pseudomonas [virulence factors and antibiotic resistance]) — Wounds (diabetes, chronic wounds) — Gas gangrene (C. perfringens, wet or dry, necrotic, pus, foul-smelling odor, much gas and pain) — Cutaneous anthrax (ulceration with a blackened center).
- Viral Infections of the Eye: Conjunctivitis (pink eye, respiratory tract infection) — Keratitis (medical emergency, Herpesvirus, lesion).
- Bacterial Infections of the Eye: Conjunctivitis (allergies, purulent, H. influenzae, C. trachomatis, N. gonorrhoeae) — Trachoma (C. trachomatis, infectious blindness, inner eyelid pebbled, trichiasis) — Ophthalmia neonatorum (N. gonorrhoeae, infected mother to newborn).
- Fungal and Parasitic Infections of the Eye: Fungal keratitis (Fusarium, Aspergillus, Candida, invasive lesions) — Parasitic keratitis (Acanthamoeba, cyst for years, photophobia, visual loss, can spread to the brain).
Chapter 20: Respiratory Tract Infections
Anatomy and Physiology
Upper Respiratory Tract: Nasal cavity, oral cavity, pharynx, sinuses, ears, larynx.
Lower Respiratory Tract: Alveoli, bronchioles, trachea.
- Tubes lined with cilia, mucus from goblet cells, mucociliary escalator rids lungs of organisms; nicotine paralyzes this mechanism.
- Bacterial infections often follow viral infections. B. pertussis slows the mucociliary escalator.
Viral Infections
Common Cold: Rhinovirus, coronavirus, influenza, respiratory syncytial virus (RSV), viral sinusitis.
Lower respiratory tract infections are called bronchitis or pneumonia (lung infection with shortness of breath and cough).
Respiratory Syncytial Virus (RSV): Single-stranded RNA virus that fuses infected cells. Severe cases can lead to bronchiolitis and pneumonia. Diagnosis requires isolating the virus; serological tests are not ideal.
Influenza: Single-stranded RNA virus. Type A causes epidemics and pandemics, Type B causes the flu, and Type C causes mild illness. Key proteins include hemagglutinin (HA), neuraminidase (NA), and M2. HA mediates attachment and entry, while NA facilitates virion release. Antigenic shift involves major RNA segment mixing, while antigenic drift involves smaller, random mutations. Classification is based on HA and NA types. Vaccines include inactivated intramuscular and attenuated nasal spray. Treatment options include Xofluza (inhibits endonuclease activity) or inhibitors of M2/NA.
Croup: Affects the larynx and trachea, causing a characteristic barking cough. Treatment includes oxygen, steroids, and humidity.
Bacterial Infections
- Otitis Media (OM): Decreased immune function can lead to epiglottitis, pneumonia, and meningitis. Common causative agents include S. pneumoniae (anaerobic, Gram-positive, alpha-hemolytic coccus with a thick polysaccharide capsule), H. influenzae (Gram-negative, requires growth factors X/V, most serious, nontypable strains are the main culprits), and M. catarrhalis.
- Bacterial Sinusitis: Often accompanies otitis media.
- Pharyngitis, Tonsillitis, Laryngitis, Peritonsillar Abscess.
- Strep Throat: Diagnosis involves exudates; treatment with beta-lactam antibiotics.
- S. pyogenes/Scarlet Fever: Causes strawberry tongue due to exotoxins.
- Strep Sequelae: M protein can mimic heart and kidney tissues, leading to acute rheumatic fever (ARF), pancarditis, valvulitis, murmur, and erythema (marginatum, annulare).
- Reemerging Upper Respiratory Infections:
- Diphtheria: Caused by C. diphtheriae (Gram-positive, lysogenized strains are toxic, affecting the nervous system and heart). Produces a thick gray membrane. Diagnosis involves scraping and immunoprecipitation. Treatment includes antitoxin and vaccination.
- Pertussis/Whooping Cough: Caused by B. pertussis (Gram-negative). Pathogenesis involves FHA/tracheal colonization factor for attachment and CyaA/PG causing fluid accumulation. Treatment includes vaccination and macrolides.
- Lower Respiratory Infections (LRIs):
- Bronchitis: Associated with smoking and COPD. Causative agents include Mycoplasma, Chlamydophila, and Bordetella.
- Community-Acquired Pneumonia:
- Atypical Pneumonia: Caused by M. pneumoniae, Legionella, and Chlamydophila. Involves multiple organs, normal white blood cell count, and gradual onset.
- Mycoplasma: Lacks peptidoglycan, has a filamentous shape, and a special tip for adherence. Common in young and old individuals. No protection against reinfection. Can cause anemia with a positive Coombs test (destruction of own red blood cells). Diagnosis via ELISA; treatment with macrolides.
- S. pneumoniae (Pneumococcus): Has a slippery polysaccharide capsule. Most common cause of pneumonia. In adults, it affects a lobe; in kids, it affects the bronchi.
- Legionnaires’ Disease: Caused by L. pneumophila (aerobic, Gram-negative, atypical). Found in water sources. Prevents phagosome-lysosome fusion (via Dot and Icm proteins). Diagnosis via BCYE/EIA; treatment with macrolides or quinolones.
- Hospital-Acquired Pneumonia (HAP)/Healthcare-Associated Infections (HAIs): P. aeruginosa (Gram-negative) forms biofilms in cystic fibrosis patients, leading to decreased sialylation, shortened”” lipopolysaccharide (LPS), and decreased toxin production. Other causative agents include Gram-negative bacteria (E. coli, K. pneumoniae, Enterobacter, Acinetobacter) and Gram-positive bacteria (S. aureus, MRSA, Streptococcus). Treatment is challenging.
- Tuberculosis (TB): Caused by M. tuberculosis (acid-fast). Particularly severe in HIV patients. Can cause abscesses in organs. Bacteria are phagocytosed but prevent phagolysosome formation, forming granulomas and lesions (Ghon complex). Decreased immune function can lead to primary or latent disease reactivation. Diagnosis via Mantoux test, chest X-ray, IGRA (if vaccinated), and NAAT. Acid-fast staining (red) is necessary as Gram staining is ineffective.
- B. anthracis: Gram-positive. Produces three subunit toxins (protective antigen (PA), edema factor (EF), and lethal factor (LF)). Not transmissible person-to-person. Death can occur within 48 hours.
Fungal and Parasitic Infections
- Fungal infections often present with vague, unrelated symptoms.
- Coccidioidomycosis: Valley fever.
- H. capsulatum: Dimorphic, causes flu-like symptoms, arthritis, and erythema nodosum.
- Blastomycosis: Affects lungs, skin, bones, and the genitourinary tract.
- Cryptococcus: Causes meningoencephalitis in AIDS patients, and can also affect the skin, lungs, prostate, urinary tract, bones, joints, and heart.
- Parasites: S. stercoralis, T. gondii, Dirofilaria, Paragonimus, E. histolytica.
- Decreased immune function and environmental factors are significant contributors.
Chapter 21: Systemic Infections
Systemic Viral Infections
- Epstein-Barr Virus (EBV/HHV4): Causes mononucleosis, transmitted via saliva. Symptoms include fever, sore throat, enlarged lymph nodes, and enlarged liver/spleen. Infects B cells. Screening involves the monospot test (latex agglutination reaction to heterophile antibody). Symptoms typically appear around 5 weeks post-exposure and resolve within 1-4 weeks. Complications include hepatosplenomegaly (with risk of rupture), jaundice, meningitis, encephalitis, renal failure, and Guillain-Barré syndrome. Associated with cancers such as Hodgkin’s lymphoma, nasopharyngeal carcinoma, and Burkitt’s lymphoma (endemic, sporadic, and immune deficiency types).
- Cytomegalovirus (CMV/HHV5): Only problematic in fetuses and immunocompromised individuals. Secondary infections occur due to low immunity. Symptoms include fever, pneumonia, encephalitis, myelitis, and neuropathy. Congenital CMV infection can lead to seizures, low birth weight, microcephaly, enlarged liver/spleen, and hearing loss.
- Other Systemic Viral Infections: Dengue: Causes joint/musculoskeletal pain; arbovirus DHF. Chikungunya Virus (CHIKV): Causes joint pain and fever. Ebola: RNA virus causing hemorrhagic fever.
- Heart Infections: Inflammation can lead to increased pressure. Viral infections are more common than bacterial. Causative agents include Coxsackievirus, EBV, Echovirus, and HIV.
Systemic Bacterial Infections
- Bacterial growth in the blood leads to sepsis, spreading through the blood to cause lymphadenitis. Septicemia occurs when the complement system is overwhelmed.
- Systemic Inflammatory Response Syndrome (SIRS): Characterized by increased or decreased temperature, tachycardia, tachypnea, and increased white blood cell count, often due to sepsis. Severe cases can affect the kidneys and heart.
- R. enterocolitica and Listeria can grow in refrigerated conditions.
- Septic shock leads to hypotension. Septic shock: Involves superantigens, microbe-associated molecular patterns (MAMPs), lipopolysaccharide (LPS) in Gram-negative bacteria, and teichoic acid in Gram-positive bacteria, leading to cytokine release, vasodilation, coagulation, hypotension, disseminated intravascular coagulation (DIC), and tissue death.
- Organisms Associated with Septicemia: Gram-negative: E. coli, Klebsiella, Enterocolica, S. typhi, F. tularensis, N. meningitidis. Gram-positive: Staphylococcus, Streptococcus pneumoniae, Enterococci, B. anthracis.
- Plague: Caused by Y. pestis, transmitted by rats and fleas. Bubonic plague leads to septicemic plague, then pneumonic plague (spread via droplets). Virulence factors include V and W cell surface lipoproteins that inhibit phagocytosis, F1 capsule surface antigen that blocks phagocytosis, biofilms, and type III secretion systems that inject proteins, disrupting the actin cytoskeleton, allowing evasion and colonization.
- Lyme Disease: Caused by B. burgdorferi, a spirochete that spreads through the blood to the skin, nerves, joints, and heart. Cleaves connective tissue. Three stages: 1) Rash, fever, headache, pain; 2) Nerve/heart involvement, joint pain; 3) Skin, nerves, synovium, neurological symptoms. Treatment with doxycycline.
- Intracellular Infections: S. typhi invades cells and macrophages, then spreads. Causes typhoid fever. Chronic carriers harbor the bacteria in the gallbladder, shedding it in feces.
- Rocky Mountain Spotted Fever (RMSF): Caused by Rickettsia. Phagocytes are infected, leading to cell bursting. Symptoms include rash, chills, confusion, and headache.
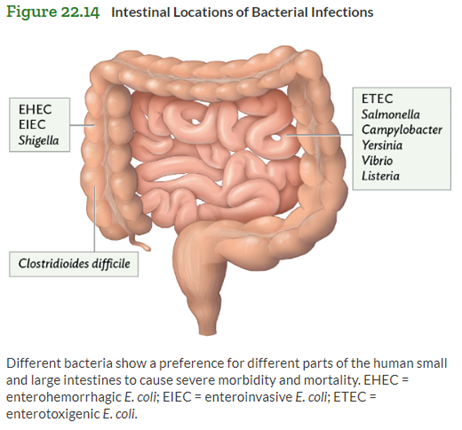
Chapter 22: Gastrointestinal Tract Infections
Anatomy of the Digestive System
Chief cells: Secrete lipase and pepsinogen (converted to pepsin in stomach acid). M cells: Microfold cells in Peyer’s patches that sample antigens from the gut lumen and deliver them to immune cells (Salmonella and Shigella enter deeper tissues through this route). Parietal cells: Secrete hydrochloric acid (HCl). Mucous neck cells: Secrete mucus and bicarbonate to form a thick mucus layer (gastric mucosal barrier).
| Oral Diseases | Viral Diseases | Bacterial Diseases | Parasitic Diseases |
|---|---|---|---|
| Tooth decay, Gingivitis, Periodontal disease, Thrush | Gastroenteritis (rotavirus, norovirus, others), Hepatitis A, B, C, D, E, Mumps | Peptic ulcer disease; Gram-negative (Gastroenteritis E. coli & Campylobacter, Shigellosis, Salmonellosis, Cholera, noncholera vibriosis); Gram-positive (listeriosis, antibiotic-associated colitis, food poisoning) | Protozoan (giardiasis, amebic dysentery, cyclosporiasis), Helminthic (whipworm, pinworm, ascariasis, hookworm, roundworm, trichinosis, schistosomiasis) |
Infections of the Oral Cavity
Normal oral flora: Streptococcus, Lactobacillus, Peptostreptococcus, Veillonella, and Diphtheroid species.
Tooth Decay and Gingivitis: Treatment often includes systemic antibiotics. Tooth decay results from plaque (biofilm) bacteria fermenting carbohydrates into enamel-dissolving acids. Gingivitis and Periodontal Disease (Aggregatibacter aka Actinobacillus actinomycetemcomitans, Porphyromonas gingivalis) involve inflammation and periodontitis (gum bleeding and recession, decreased bone density), potentially leading to trench mouth (Vincent’s angina – necrotizing – grey film, abscesses, bad breath). Thrush (Candida albicans) is treated with Nystatin (antifungal), common in neonates and infants (cottage cheese-like patches on the tongue), and can be a secondary infection in adults on prolonged antibiotics or with weakened immune systems.
Gastrointestinal Syndromes
Types of Diarrhea: Enables rapid pathogen dissemination. Osmotic: High intestinal osmolarity draws out water (similar to lactulose, rotavirus). Secretory: Electrolyte over-excretion (cholera). Inflammatory: Cytokines attract polymorphonuclear leukocytes (PMNs), damaging the intestine and decreasing absorption, leading to bloody diarrhea and dysentery (Shigella, Salmonella). Motility-related: Increased motility and decreased absorption, caused by enterotoxins (e.g., rotavirus).
Types of Inflammation: Gastroenteritis (non-specific term). Gastritis (stomach lining). Enteritis (small intestine). Enterocolitis (colon and small intestine). Colitis (large intestine/colon).
Viral Gastroenteritis: Vaccines available for Hepatitis A (HAV), Hepatitis A and B combination (HAB), Rotavirus, and Mumps. No vaccines for Hepatitis C (HCV), Hepatitis D (HDV), and Norovirus.
Hepatitis: Causes: Infection, alcohol (EtOH), toxic chemicals, some medications (including Tylenol), autoimmune conditions, pathogens (viruses, amebas, worms). Symptoms: Enlarged, painful liver, jaundice, dark urine (bilirubinuria), clay-colored stool, fever, nausea and vomiting, weight loss. Diagnosis: Elevated liver enzymes aspartate aminotransferase (AST) and alanine aminotransferase (ALT). Hepatitis A: Anti-hepatitis A virus (anti-HAV) IgM for acute infection or IgG for previous infection. Hepatitis B: Hepatitis B surface antigen (HBsAg), Hepatitis B e antigen (HBeAg), anti-hepatitis B virus (anti-HBV) IgM. Hepatitis C: RNA molecular assay. Hepatitis D: Polymerase chain reaction (PCR) for RNA, serum IgG and IgM. Hepatitis E: Flu-like symptoms, IgM via enzyme-linked immunosorbent assay (ELISA), virus in bile/stool/hepatocytes. Risk of cancer/cirrhosis with Hepatitis B and C; fulminant hepatitis with Hepatitis D. Hepatitis D only occurs with Hepatitis B. Transmission: Fecal-oral (Hepatitis A and E), parenteral/sexual (Hepatitis B, C, and D), food (Hepatitis A), vertical (Hepatitis E). Treatment is mostly supportive care, except for interferon-alpha (IF-alpha) for Hepatitis B, C, and D, antivirals for Hepatitis B and D, ribavirin for Hepatitis C, and liver transplant for Hepatitis D. Vaccines available for Hepatitis A and B. Onset: Abrupt for Hepatitis A, D, and E; insidious for Hepatitis B and C. Hepatitis B virus codes for 4 viral proteins.
Mumps: Paramyxovirus with single-stranded RNA; highly infectious, spread via saliva/droplets. Parotid gland infection is self-limiting and leads to immunity. Mechanism: Replicates in the upper respiratory tract, then migrates to the parotid gland via the blood. Symptoms: Flu-like symptoms 2-3 weeks post-infection, parotiditis, pain with chewing/swallowing. Sequelae: Meningitis, encephalitis, testicular swelling (orchitis) with potential atrophy/infertility, ovarian swelling (oophoritis).
Rotavirus: Non-enveloped, segmented, double-stranded RNA, highly infectious via fecal-oral spread. Incubation period of 2 days. The virus attacks the intestinal epithelium, resulting in osmotic diarrhea that is green due to bile. Produces enterotoxin leading to hyperperistalsis and vagus stimulation (nausea and vomiting).
Norovirus (Norwalk/stomach flu): Non-enveloped, positive-sense, single-stranded RNA; outbreaks common in crowded areas (e.g., cruise ships) via fecal-oral spread. Incubation period of 24 hours. Symptoms: Sudden onset of vomiting, abdominal cramps, watery diarrhea, flu-like symptoms (headache, fever, chills, muscle aches). Treatment is supportive care.
Bacterial Infections of the Gastrointestinal Tract
-Gram-Neg: E. coli, Shigella, Salmonella, Yersiniosis, Campylobacter Enterocolitis
-Gram-Pos: Listeria monocytogenes, C. Diff, Staph aureus
Gram-neg bacteria
Escherichia Coli Gastroenteritis: acid-resistant; 10-100 organisms can cause disease. 6+ different diarrhea-causing pathovars (classes), differentiated by their O (part of LPS) and H (flagellar protein) cell-surface antigens. General mech: attach to host cell via pili, EHEC/EPEC use syringe-like type III secretion system to signal protein synth to host cells. Cytokine secretion → loss of microvilli (attaching & effacing lesion), diarrhea. Specific mech; Sx: ETEC (secretes labile toxin, with action identical to cholera toxin; secretory D); EIEC (invades epithelial, similar to Shigella; bloody w fecal WBC); EHEC O157:H7 and similar cause serious disease; bloody; bacteria can reside in intestines of cattle and others). No animal reservoirs: ETEC, EIEC; FO ETEC, EIEC, EHEC. STEC: blanket term for Shiga toxin-producing E.coli
HUS (hemolytic uremic syndrome) and TTP (thrombotic thrombocytopenic purpura): Shiga toxins 1 and 2 cleave host ribosomal RNA, halting protein synthesis and killing host cell. Results in clot formation (thrombocytopenia), vessel occlusion. Called HUS in kidney (decreased urine output, increased fluid retention and puffiness); TTP when systemic (Sx petechiae and purpura, neuro symptoms). Tx: supportive, blood transfusion, dialysis. **Abx not recommended (can trigger HUS)
Shigellosis (bacillary dysentery): Acid-resistant. similar mech to EIEC but lack flagella (H antigen) so non-motile. 45 antigenic serotypes (groups A-D). Invade using type III secretion system. S&S: 1-4D incub, then cramping, fever, vom, anorexia, watery diarrhea, then tenesmus (urge to defecate), fecal incontinence, mucoid diarrhea with red blood. Tx: supportive, Abx (quinolone)
Salmonellosis: systemic (S. bongoriin cold-blooded animals, S. entericaotherwise has thousands of serovars) that cause (1) typhoid/enteric fever. FO transmission; no animal reservoir. S&S 1-3w following ingestion, stepwise fever>40, bacteremia, abdo pain, rose spots (salmon-coloured rash) on abdo/trunk, diarrhea/constip, hepatosplenomegaly, septic shock. Tx: Abx (fluoroquinolones, ceftriaxone) (2) enterocolitis/enteritis spread thru animal contact. S&S 6-48 hrs n&V, diarrhea, fever. Tx: Abx if septicemic. (3) Asymptomatic carriers of S. Typhi which evades immunity via virulence antigen capsule. Tx: 4W amoxicillin or trimethoprim-sulfamethoxazole.
Yersiniosis (Yersinia, bacilli, infect M cells) Y. enterocolitica: food/milk transmission. (causes enteritis/enterocolitis). Self-limiting unless it infects mesenteric lymph nodes or it turns systemic, in which case Abx (aminoglycoside, quinolone, 3rd gen cephalosporin) Y. pseudotuberculosis (penetrates intestinal mucosa, leading to septicemia, metastatic infections of organs; no diarrhea). Survives and multiplies in/out of fridge
Campylobacter Enterocolitis (C. jejuni and C. coli, corkscrew): live in intestinal microbiota of poultry and cattle. Leading cause of diarrhea. Disseminated (multi-organ) disease in immunocompromised. Can lead to Guillain-Barré syndrome (demyelination). Bloody diarrhea. Invades M cells. Naturally resistant to Abx (penicillins, trimethorprim, most cephalosporins); sensitive to macrolides and fluoroquinolones.
Vibrioses (1) Cholera: (curved rod, acid-sensitive) lives in brackish waters. Secretory rice water diarrhea (10-15L fluid per day loss). Secretes cholera toxin in small intestine. Non-invasive: no fever, no fecal blood, no WBC. Tx: self-limiting with fluid replacement (or doxycycline). Two oral vaccines available (not widely used) (2) Non-cholera: V. parahaemolyticus found in undercooked seafood and V. vulnificus (high sepsis risk)
Gram-pos bacteria Listeria monocytogenes (listeriosis). Spread by food (unpasteurized raw milk, processed food), vertical tx; survives at high and low temps. Actin-based motility. Lives inside macrophages. Can cross BBB. Can be mild to severe. Tx: ampicillin. NO vaccine. C. diff: antibiotic-associated colitis (due to lack of bacterial competition). Forms yellowish plaques of sloughed-off intestinal epithelial cells, blocking intestinal absorption. Produces A, B, CDT toxins that can loosen tight jxns and ↑TNF-a prod’n (↑inflammation), leading to pseudomembranous colitis. Tx: Metronidazole, Vancomycin, probiotics, fecal transplant, colectomy Staph aureus. Spread in foods esp at picnics. Its heat-stable enterotoxins stimulate nerve in the vomit centre of the brain. Onset 2-6 hrs, resolved 24-48 hrs.
22.6Parasitic Infections of the Gastrointestinal Tract
Protozoa (paramecia and amebas): enter body as a cyst. Giardiasis (flagellated, anaerobe). Tx from animals (rodents, deer, cattle, pets). Produces trophozoite in GI. Greasy/watery stools. Tx metronidazole. Amebiasis (amebic dysentery). Forms cysts (4 nuclei) or trophozoites (1 nucleus). Often harmless unless protozoa penetrate mucosa after 2-6W. Tx iodoquinol, metronidazole if disseminated disease. Cryptosporidiosis (C. hominis, C. parvum) Spread via animal waste in drinking or chlorinated water. Oocysts dissolve and release sporozoites then reproduce. Dx acid-fast stain, direct immunofluorescence, immunoassay. Tx oral rehydration, nitazoxanide. Self-limiting but severe illness with AIDS (retroviral prophylaxis). Cyclosporiasis: Ingested in fresh produce and contaminated water as an oocyst with shell. Shell dissolves in GI, freeing sporozoites. Illness 1-2 weeks post-exposure. Tx trimethoprim-sulfamethoxazole.
Helminths (worms); 0.3mm – 25 m; (1) Roundworms (nematodes); Flatworms (platyhelminths) (2) Flukes (trematodes) (3) Tapeworms (cestodes); S&S d/t immune response (↑Eosinophils). Dx: Eosinophilia in peripheral blood & ID of eggs in stool. 4 lifecycles (Fig 22.29) Transmission routes: A (FO, Trichuris, Enterobius, Ascaris); B (F-env-skin, Necator americanus, Ancylostoma duodenale), C (F-int. host-O. Taenia, Diphyllobothrium, Echinococcus), D (A-B combo, Schistosoma, Opisthorchis). All life cycles require definitive host (where they lay eggs); C &D require intermediate host. Tx: varies with organism, and doesn’t ensure complete elimination d/t poor systemic absorption
4 categories of disease: (1) Intestinal Distress: Cycle A (Whipworm, Trichuris trichiura, can cause dysentery, ↓ muscle tone, protruding rectum; Pinworm, Enterobius vermicularis, common in children, causes anal itching (& reinfection), diarrhea). Tapeworm, Taenia (saginata – beef, solium – pig), diphyllobothrium latum (fish); head is scolex, body proglottids; sx nausea, abdo pain, proglottids in feces, weight loss. (2) Intestinal Distress + Larval Migration Sx: Ascariasis, Ascaris lumbricoides (most common nematode) can travel to lungs, cause bowel obstruction, appendi/peritonitis. Hookworms (Necator americanus, Anculostoma duodenale) nematodes, Cycle B, enters skin (itchy dermatitis), travels to lungs and mouth (transient pneumonia), GI pain and diarrhea. Main Sx is ↓Fe. Strongloidiasis Strongloides stercoralis B-type cycle, two forms, filariform is infective, travel to lungs and mouth, capable of parthenogenesis (reproduce w/o males), causes strongyloidiasis (itchy, serpentine, red rash; higher risk with immunosuppressant use; can travel to liver, kidney, CNS. (3) With muscle involvement: Trichinosis (in meats, esp pork) ingested cysts free larvae that reproduce and newly hatched larvae invade muscles and turn into cysts. Once in muscles, uncurable. (4) With liver involvement: Cycle D (Schistosoma, Fasciola), penetrate skin and evade immunity by coating bodies with host blood proteins. Opisthorchis flukes, ingested from fish, migrate from intestine to bile duct; usually asymptomatic.
Chapter 23 (23.2. 23.4. 23.5)- (Elisa)
23.2 Urinary Tract infections
UTI
more common for women
Most common nosocomial infection- HAI: Catheter assoc. UTI
Cystitis: bladder infection
Dysuria, increased freq. Of urine, urgency, burning
Complications: acute pyelonephritis, bacteremia, sepsis
Pyelonephritis: kidney infection
Arise from bladder infection by microbes that ascend the ureter/occasionally from septicemic blood- symptoms of lower urinary tract infection, cloudy foul smelling urine
High fever, oliguria, costovertebral tenderness (palpate back)
and nauseaComplications: kidney necrosis/abscess, sepsis, preterm labour
E coli, staphylococcus saprophyticus
Klebsiella, proteus, enterobacter, clostridium, candida in diabetes
Pathogenesis of UTI
Infection from urethra to bladder
Bacteria residing along the superficial urogenital membranes of the urethra can ascend to the bladder. This route of infection is more common in women than in men.
Ascending infection to kidney
Organisms from an established infection in the bladder ascend along the ureter to infect the kidney.
Descending infection from the kidney.
Bacteria can travel via the ureters from the infected kidney into the bladder. Kidney infections may arise when microorganisms are deposited in the kidneys from the bloodstream.
**Urine is bacteriostatic to most of the Gram-positive microbiota inhabiting the perineum and the vagina, such as lactobacilli, corynebacteria, and Staphylococcus epidermidis.
The most common etiologic agents of UTIs are the uropathogenic E. coli (75% of all UTIs), Klebsiella, Proteus, Pseudomonas, Enterobacter, Staphylococcus aureus, Enterococcus, Chlamydia, fungi, and Staphylococcus saprophyticus
Antibiotic therapy is recommended: eg; trimethoprim-sulfamethoxazole
Increase fluid intake, cranberry juice
Symptomatic bacterial UTIs are treated with antibiotics such as trimethoprim-sulfamethoxazole.
Lower urinary tract infection: usually afebrile except in young children
UTI in early life are preventable in children less than 6 months old and uncommon in children over 12 years of age
Older adults: atypical symptoms like delirium
Urinalysis has three parts: determining the color and clarity of the sample, microscopic examination, and biochemical studies performed with a dipstick, also called a dry reagent strip
Asymptomatic Bacteriuria
Bacteria in urine often with no signs/ symptoms: greater than 10^5 organisms/ml of urine
Concern for pregnant women
Assoc. Low birth weight of newborn, preterm labour, perinatal death
23.4 Sexually Transmitted Infections of Reproductive Tract
VIRAL STI
Genital warts
Symp: soft tissue growths- recurrent- cauliflower-shaped- on rectum/genitals
Virus: Human papillomavirus- HPV
Dx: Clinical presentations, biopsy
Treatment: removal of warts: surgery, cryotherapy, med (podofilox)
Prevention: HPV vaccine, condoms
Genital Herpes
Symp: Cluster of erythematous papules and vesicles, burning, pain, itching, fever, H/A muscle pain, dyuria
Virus: Herpes simplex virus (HSV-2, HSV-2)
Dx: Clinical manifestations, viral culture, PCR, serology
Treatment: antiviral meds, diff treatment methods for first/ recurrent episodes and suppression
Prevention: No vaccine, condoms
Neonatal Hepes
Pregnant mothers with HSV can vertical transmit to baby
Skin infection with small fluid filled vesicles-can rupture, crust over and heal
Can spread through blood stream: affect brain, lungs, liver and kidneys
Cyanotic, tachypnea, jaundiced, hypothermia, bleed easily
HIV/AIDS
Symp: Primary infections: No symp, some may have acute illness with fever, muscle and joint pain, lymphadenopathy, rash on trunk
Symp depends on progression
Virus: Human immunodeficiency virus (HIV)
Dx: ELISA, nucleic acid test HIV, p24 antigen test, viral cultures
Treatment: antiretroviral therapy- CD4+ T-cell count and viral load
Prevention: No vaccine, condoms
Lentivirus win RNA genome- retroviridae family
Sexually transmitted or through bodily fluids
NOT through kissing, tears or mosquito bites
AIDS
Pneumonia: pneumocystis jirovecii
High fever, diarrhea, some cancers, peripheral neuropathy
Secondary infections: persistent vaginal candidiasis,listeriosis, shingle
BACTERIAL AND PROTOZOAN Infections
Syphilis
Symp:Primary:chancre- painless ulcer; Secondary: gen. Rash, gen. Nontender lymphadenopathy, fatigue, fever; Tertiary: loss of coordination of movement, progressive dementia, stroke, CNS abnorm. Abnorm.pupillary rx to light, gummas, thoracic aortic aneurysm
Organism: Treponema pallidum
Dx: dark field microscopy and detection of organism in lesion/ tissue sample
Treatment: benzathine penicillin G (BPG), azithromycin,
Gonorrhea
Symp: F- gonococcal cervicitis: no symp; may have vag. Discharge, dyspareunia, vag bleed after sex; M- gonococcal urethritis: mucopurulent/purulent discharge, dysuria, urethral itching
Organism: Neisseria gonorrhoeae- gonococcus
Dx: >5 WBC in gram stain or urethral discharge- gram neg. Diplococci
Treatment: ceftriaxone, doxycycline
Nongonococcal urethritis
Symp: dysuria, urethral discharge itching
Organism: chlamydia trachomatis (most common), mycoplasma genitalium, adenovirus, herpes simplex virus
Dx: >5 WBC in gram stain or urethral discharge- gram neg. Diplococci, + leukocyte esterase test on first void urine
Treatment: Azithromycin, doxycycline
Lymphogranuloma venereum
Symp: unilateral tender inflammation of groin lymph nodes, constipation, anal pain and discharge is anal exposure
Organism: chlamydia trachomatis
Dx: Culture of swab of lesion, direct immunofluorescence test
Treatment: Doxycycline
Chancroid- soft chancre
Symp: acute +++ painful multiple genital ulcers- papules/pustules
Organism: Haemophilus ducreyi
Dx: Iso of organism in culture from genital ulcer samples
Treatment: azithromycin, ceftriaxone, ciprofloxacin, erythromycin
Trichomoniasis vaginitis
Symp: F- copious malodorous vag discharge, vulvar itching and burning; M- aysmp or urethritis symp
Organism: Trichomonas vaginalis
Dx: culture for organism from vag discharge/ urethral swab
Treatment: metronidazole, tinidatzole
23.5 Non- sexually Transmitted Infection of the Reproductive Tract
Bacterial Vaginosis- BV
Symp: foul smelling discharge
Organisms: gardnerella vaginallis- maj. Casue, mycoplasma hominis, peptostreptococcus spp.
Fournier’s gangrene
Symp:Prodromal fever 2-7 days pr → wounds with drainage and gangrene
Organsims: polymicrobial necrotizing fasciitis – anaerobic organisms, enterobacteriaceae, streptococcal, stephylococcal and stephylococcal species and fungi
Vulvovaginitis
Symp: acute vag discharge, vulvar itching and pain→ dysuria
Oragnism: Candida albicans (80%–92%) and other Candida species; overgrowth of personal microbiota after immunosuppression, hormonal changes, trauma, or antibiotic therapy
Chapter 24, (24.2, 24.3. 24.4)
24.2
severe->death
Early s/s:flu-like, HA,dizzy,fatigue, then worsen
Late: edema->^ICP, paresthesia, hyperesthesia, areflexia, altered mental state/memory
Route: distal to brain, or from adjacent bone/structure.
Dx: bld/csf
3 diseases. Meningitis: inflamm meninges (HA, fever, confused)
Encephalitis: inflamm brain, often s/s: CSM. Primary: direct; secondary: from elsewhere
Viruses: myelitis (inflamm spinal code) radiculitis (spinal nerve root)
Dx: pleocytosis (WBC in CSF)(PMN: bact; lymphocytes: virus); protein? Dmg
WBC | glucose | protein | |
Normal | 0-5 | 40-70 | 15-50 |
virus |
| N | N |
bact | 100->1000 | low | Elevated |
fungal | varies | low | Slight elevate |
Tx: lower inflamm; bact: antimicrobial. Vaccines (not many) or prevent ie via fumigation
24.3
Most viruses->aspective meningitis (no bact)
Table?
Rabies: -ve sense, ssRNA, bullet shaped. VSV (flu, oral lesions) and rabies
Neurotropic virus. Inf. local nerve -> brain. 3 types
‘furioous(hydrophobia), paralytic, atypical (neuropathic pain, sense/motor, breathing)
Dx: antigenic typic, nucleic acid. qRT-PCR->bld/CSF. Postmortem? Negri bodies
Tx: Ig, vax ASAP
Mosquito encephalitis
EEE: +ve sense, ssRNA, arbovirus (insects), rare, deadly. Dx: antibody titer >4X
WNV: +ve sense, ssRNA, mosquitoes. Zika virus (microencephaly fetus)
Viral meningitis: HA, fever, photophobia, muscles, malaise
Mostly enterovirus; +ve sense, ssRNA. Often
LCMV: enveloped, -ve sense, ssRNA. Mice. cause asep men, enceph, menenceph. Dx: very high lymphocytes. s/s: 1:flu, 2: stiff neck. Vertical transmission
Poliomyelitis: fecal-oral, saliva. GI->brain, 1-3 weeks. phrenic nerve (diaphragam).
Postpoliosyndrome (PPS) 30-40 years later, insidious, non-shedding. Tx: s/s, PT.
Dx: virus in stool AND cytopathic effect
Salk vax: inactivated. Sabin vax: attenuated, oral, can -> VAPP
24.4
Affect old/young
Table
Bact meningitis: s/s: nucchal rigidity. Can cause systemic as well
3 bacts: s. Pneumonia (yng/old), n.meningitidis (young adult), L. monocytogenes (preg, old). Dx: hx, CSF, gram stain
Meningcoccoal meningitis: G -ve, diplococcus. Throat. Type IV pili, to bld. Modified LPS, called LOS, grows blebs(endotoxic)->circ->^permeability&lowers platelets-> petechiae->pupura
Has capsule, avoids complement. Adheres to BBB, loosens, squeezes thru.
Capsule types, used to dx, B=sporadic inf, A,C,Y,W135: epidemic. Has vax. Contagious so prophylactic tx
Listeriosis: G +ve, facultative, anaerobic rod & intracelluls pathogen. Survive cold, actin tail, infect fetus -> death. So preg w/bachache? Take diet hx. Tx: antibiotic, dx:CSF
Neonatal meningitis: vaginal or vertical, often e.coli & group b strep. Dx mom@35-37weeks. Fetus s/s: neuro, fever, NV. dx: G stain, CSF. tx: antibact
Bact neurotoxins: light chain disrupts NT’s
Tetnus: excessive signalling, blocks GABA; lockjack; from dirt
Botulism: obligate anaerobe (canning, honey), blocks acetylcholine (flaccid paralysis)
Chapter 25
25.1
Sample collection (C=culture, TT=toxin test, AB=antibody, A = antigen)
BACTERIA C. diphtheria (nose, throat C, TT), B. pertussis (nasopharyngeal smear w/ fluorescent AB, ELISA for respiratory secretions), Leigonella pneumophila (C, PCR for nuc. acid, enzyme immunoassay for urine A), Campylobacter spp. (stool C, microaerophilic condition), Leptospira interrogans (serological tests pre/post illness 2-3 weeks for AB), Listeriosis (C blood, spinal fluid, DNA probe), Chlamydia trachomatis (monoclonal AB for urine pus A, nucleic acid probe) Treponema palidum/syphilis (fluorescent AB stain tissue), Francisella tularensis/tularemia (C blood on cysteine medium, fluorescent AB stain pus, AB titer), Y. pestis/plague (fluorescent AB, ELISA, PCR, IgM serology)
VIRUSES Rhinovirus (AB from nasal secretions), Influenza (rapid A, viral C of nasal sec., qRT-PCR, compare AB blood in acute/convalescent stage of illness), Hantavirus/pulmonary syndrome (electron microscope, monoclonal AB for tissue, ELISA, Westernblot for IgG, IgM in blood), HSV (viral C, fluoresc. AB, DNA probes), Mumps (serum AB, presence of IgM in blood, viral C), Rotavirus/diarrhea (ELISA stool, qRT-PCR), HIV/AIDS (AB in blood, Western blot, PCR), COVID19 (qRT-PCR for nucleocapsid gene, AB nucleocapsid, antigen detection)
FUNGICoccidioides immitis/coccidiomycosis (PCR, large, thick walled, round spherules in clinical specimens) Histoplasma capsulatum/histoplasmosis (examine stained material, AB blood, A urine or blood)
Sterile samples: blood (S. epidermidis, C. acnes common contaminants, presence of organism in blood from two body sites = most likely causative agent) CSF (lumbar puncture/spinal tap, centrifuge and stain sediment + test for increase protein and decreased glucose), pleural/synovial/peritoneal (aspirated & cultured, view for inflammatory cells). Sites w/ normal microbiota skin/throat/nasopharyngeal (sterile scalpel + 10% KOH potassium to dissolve tissue and observe fungus, viral lesion -> transfer to virus transport medium rushed to lab)
Supplmentary COVID (Louis)
SARS-CoV-2 is in coronavirus family, all with ssRNA genome and envelope. Replication steps: 1. Virus binds to ACE2 receptor on cell, 2+3. Translation of viral protein & Transcription of RNA genome 4. ER+Golgi complex assemble virus w/ genome, viral and nucleoproteins, 5. Exits host cell
Transmission: indirect contact (fomites: thru objects) + direct contact (mostly airborne). Droplets linger 2-4hrs, inactivate in 8-20 min by UV
Phases: Incubation (replication before symptoms): 5-6 days, up to 14d. Illness: 2 weeks, 10% symptoms beyond, 90% w some symptoms 60d later. Decline: symptoms improve but still infectious. Stopping Isolation conditions: no fever 24h + symptoms improved + 10 days since symptoms appeared
Enters resp. Tract, infects cells of resp tract, but also heart, kidney, small intestine. Harm is caused by lysing cells from ACE2 receptor binding of above + immune/inflamm. Response. Prevents binding of endogenous ligands.
Detection: detect virus components, detect Ab for virus proteins in serum. W/ special RT-QPCR, taq polymerase extends viral RNA and causes fluorescence signal
Rapid/point-of-care test: mucus or blood sample added, Abs+virus proteins from host are trapped by Ab on slide, causing color change, unbound Abs are captured and cause control line to show
25.2-25.5 (Karol) *based on the section objectives
Biochemical Profiles for Pathogen ID
-Use profiles and algorithms for identification.
Gram-Negative vs. Gram-Positive
-Major features differentiate them biochemically.
Lancefield Classification
-Key for grouping beta-hemolytic streptococci.
Selective vs. Differential Media
-Selective: Inhibit some, allow others.
-Differential: Spot differences.
Acid-Fast vs. Gram Stain
-Acid-fast: IDs mycobacteria.
-Gram: Differentiates bacteria by cell wall.
Mass Spectrometry for Pathogen ID
-Rapid ID via whole-cell protein profiles.
25.3
1. Polymerase Chain Reaction (PCR) in Pathogen Identification
-PCR amplifies DNA, detecting pathogens in clinical samples.
-Real-time PCR: Monitors DNA amplification in real-time, aiding clinical diagnosis.
2. Advantages and Disadvantages of Pathogen Identification Methods
PCR:
Advantages: Sensitivity, speed, specificity.
Disadvantages: Costly, risk of contamination.
Restriction Fragment Length Polymorphisms (RFLP):
Advantages: Differentiates strains, cost-effective.
Disadvantages: Time-consuming, requires skilled technicians.
Biochemical Strategies:
Advantages: Cultures organisms, identifies biochemical properties.
Disadvantages: Slow, may miss non-culturable pathogens.
25.4
Enzyme-Linked Immunosorbent Assays (ELISA)
-Identifies microbial antigens in clinical samples or antibodies in serum.
-Uses enzyme reactions for detection, quick and sensitive.
Fluorescent Antibody Staining Technique
-Stains microbes with fluorescent antibodies.
-Visualizes under fluorescence microscope, rapid identification.
25.5
Assay Specificity vs. Sensitivity
-Specificity: Measures test accuracy for true negatives.
-Sensitivity: Measures test accuracy for true positives.
Immunochromatography Assay
-Point-of-care diagnostic kits use this assay.
– Rapid detection based on antigen-antibody interactions.
Advantages and Disadvantages of Point-of-Care Diagnostics
-Advantages: Rapid results, on-site testing, easy to use.
-Disadvantages: Limited sensitivity, potential for false positives/negatives.